For a medical student, anatomy lab is a rite of passage.
Everything about it is a test: Can you withstand the sharp sting of formaldehyde at 8 AM? Can you differentiate between the vagus and the phrenic nerves? Can you delicately dissect the muscles of the forearm?
Can you make that first cut?
Human emotion fascinates me and my psyche just so happens to be a complex, peculiar, and interesting specimen to study. The psychological effects of working in the anatomy lab had a profound impact on me, even with scalpel in hand two months after my first day. Day one of lab went just as I had anticipated: I kept my cool until someone broke my composure by casually asking how I was doing. I fought back tears after the harmless inquiry until I could isolate myself and let it all out in a corner between a large window and a countertop covered in plastic model brains. I had been trying to make a positive first impression on my lab group by keeping a composed demeanor despite being in an environment worthy of vast displays of emotion. Clearly, this was no simple task. Although mixed with a bit of embarrassment, I immediately felt relief upon the crumbling of the emotional dam that I had worked so hard to build. I would have stayed in the corner longer to release all of the fear, sadness, and confusion had I not felt so guilty about leaving my group within the first five minutes of lab. I typically use distraction techniques to rid myself of negative thoughts but the impending return to the lab table invalidated those tricks. Instead, I accepted that I had nothing to be embarrassed about, that I could sort through my feelings on my bike ride home, and that it is okay to let my classmates see me cry. One deep, cleansing breath later, I rejoined my group and together we embarked on our seventeen-week journey.
After that episode, I dreaded returning to the chilled tank that housed the body of a woman who could have been my mother: same age, same surgical scars, same body type. In the seven-day interim, I pondered her life. I wondered about her family, where she had worked, what made her choose to donate her body. I wondered if she died in peace or in pain. I thought about the people in my life who had passed away. Each of their deaths was sudden, painful, unanticipated, and unjustified, and left me with an incredibly significant sadness. I wondered if my perspective on death was natural, if it was normal for me to feel such heartache in the presence of a deceased stranger. I eventually concluded that there is no perfect answer because there is no norm by which to judge my perspective. With that understanding, I made peace with my emotions.
My sadness subsided over the subsequent weeks as I found myself head-over-heels in amazement and respect for the human body. I felt like a pilgrim finally reaching a sought-after shrine, seeing for the first time with my own eyes the conglomerate of vessels, nerves, organs, and muscles that until then I had only ever read about. Despite the body’s collective complexity, the individual parts seemed unbelievably simple and incapable of carrying out the multitude of physiological functions required for life.
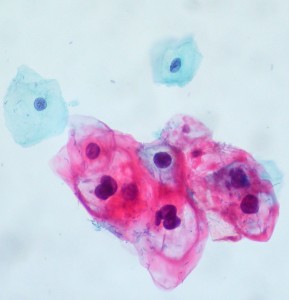
As we uncovered one pathologic finding after another in our hunt to determine our cadaver’s cause of death, I began to involuntarily formulate a mental scenario of this woman’s final years, months, and even the day she died. Soon enough, each physical finding that suggested a potential cause of her death was accompanied by an imagined reproduction of her life. One half of me was determined and anxious to uncover new pathology that might lead to a stronger differential and the other half wished it could painlessly declare natural causes. In the histology lab, I encountered yet another emotional challenge. One minute I was eagerly anticipating visible signs of liver metastasis and the next I was welling up behind the eyepiece of my microscope, imagining our young patient receiving the news that she had five months to live.
No two medical students have the same anatomy lab experience. For me, the past nine weeks have altered my view of death and further sensitized me to human suffering. Death no longer seems personal, but rather a fundamental biologic process. It is the suffering that often precedes death that has consumed me as an anatomy student. Death undoubtedly brings about a suffering all its own—which was my initial source of heartache at the beginning of lab season. Who did this woman leave behind? Are they still grieving over her passing? But as we uncovered her countless medical problems, I wondered what was harder for her family and friends: to live with her absence, or to live with her suffering?
When it comes to anatomy lab, many medical students would express that there is nothing to it — it is simply another requirement. For others, it is unashamedly so much more. It is said that the cadaver is the medical student’s first patient. I only wish I had the opportunity to thank mine.
Featured photo courtesy of UC Davis School of Medicine