In November 1999, the Institute of Medicine released a study entitled “To Err is Human: Building a Safer Health System.” Within the first line of that study, a sobering statistic was revealed: between 44,000 and 98,000 hospital deaths each year are attributable to preventable medical errors.[1] We have been taught about the communication shortcomings that can easily occur between members of a medical team who may be stressed, sleep-deprived, rushed. Even though we have been warned about the potential dangers that can result from the use of abbreviations and imprecise communication, it took a recent misunderstanding for me to leave my Boards-bubble and comprehend, on a personal level, just how misleading certain abbreviations can be.
A few weeks ago, I sat down at my desk and began going over the first lecture of the day. This was 6:30 am: pre-coffee, pre-sunlight, pre-hair combing. At the time, we were studying the gastrointestinal system. As I reviewed the first few slides of this lecture, I became very confused. I kept seeing the abbreviation ‘LES,’ and I really couldn’t figure out what it was referring to – you have my full permission to laugh at me right now; like I said, it was pre-coffee. As a born and raised East Coaster, LES means one thing and one thing only to me: the Lower East Side of Manhattan. If you are unfamiliar with New York City, please allow me to take a brief detour here to tell you a bit about the wonders of the Lower East Side (LES). The LES has a rich history, greatly influenced by the fact that many Eastern European immigrants settled into tenement housing in the area after coming through Ellis Island. When I think of the LES, I think about deli sandwiches that are too large to fit through a human mandible, knishes, amazing donuts, and macaroni and cheese pancakes. I do not reflexively think about acid reflux, vomit, and esophageal cancer, although the association may make sense considering the indulgent foods just mentioned. As you might imagine, when I finally figured out that LES was intended to stand for ‘lower esophageal sphincter,’ it was a bit of a letdown. And since I couldn’t get the aforementioned amazing donuts out of my head, my whole morning was pretty much lost when I spent 45 minutes on the phone trying to coordinate a cross-country delivery of them to the West Coast.
Despite the ambiguity, and in my case, potential hilarity, of using abbreviations, one thing is clear: there is an abundance of statistics and data to back up the assertion that medical errors cost lives. Just run a Google search for ‘medical error abbreviation deaths’ or some variation thereof and you will see thousands of hits about the health hazard of medical miscommunication. It’s easy enough to find data showing how detrimental some timesaving charting techniques can be. As newly-minted members of the medical profession, we have the responsibility to act as the new guard and to usher in safer communication and documentation practices. We can begin to advocate for better safety practices by trying to limit our use of abbreviations in our charting, and we can ask our professors to do to the same in their lectures and test questions. Though becoming a physician is a long and rigorous journey, we should never take shortcuts along the way that have the potential to put our patients at risk of harm.
While attending a residency application question and answer meeting, I learned that 2016 marks the first year in over a decade that my mentor will not be taking medical students on an international health elective. She emphatically explained that it would be unethical to expose students to known Zika virus-infected areas, and irresponsible to potentially create a reservoir of Zika virus to bring back to the United States. Her second point resonated with me, because I had just examined a patient in clinic who commutes every two weeks between Puerto Rico and Orlando, Florida. He is a 30-year old male who engages in sexual activity with women only and reports inconsistent condom use. This worries me.
Puerto Rico has been hardest hit by the Zika virus pandemic, and is ground zero for Zika virus infection in the United States and territories. Between index case documentation on November 23, 2015 and January 28, 2016, there were 155 suspected Zika virus disease cases in Puerto Rico (Thomas, 2016). As of May 18, 2016, there are 544 reported travel-associated Zika virus disease cases (10 sexually transmitted; 1 Guillain-barré syndrome) in the United States and 0 locally-acquired vector borne cases (http://www.cdc.gov/zika/geo/united-states.html). The U.S. Zika virus infection in the United States and territories (USZPR) and the Zika Active Pregnancy Surveilance System (ZAPSS) registries are tracking cases of pregnant women with any laboratory evidence of possible Zika virus infection in the U.S. and territories, and reporting data every Thursday at the following website: http://www.cdc.gov/zika/geo/pregwomen-uscases.html As of May 12, 2016, there were 157 pregnant women in the U.S. and District of Columbia with laboratory-suspected Zika virus infection.
Zika virus can spread from a pregnant woman to her fetus and is known to cause microcephaly and other brain abnormalities (ACOG Practice Advisory, March 31, 2016). The virus can also be transmitted through unprotected sex with a male partner, spurring the Centers for Disease Control and Prevention (CDC) HAN (Health Alert Network) advisory for the prevention of sexual transmission of Zika virus (Oster, 2016). Clinical criteria for Zika virus disease include the presence of (Simeone, 2016):
Guillain-Barre syndrome;
OR
in utero findings of microcephaly or intracranial calcifications in a mother with clinically compatible symptoms or epidemiologic risk factors (eg. sexual activity with a known Zika infected man) for Zika virus infection;
OR
one or more of the following symptoms
fever;
rash;
arthralgia;
conjunctivitis
Zika virus disease is not the first maternal virus infection to cause or be associated with congenital abnormalities, but it is the first known mosquito-borne infection to cause congenital anomalies in humans. The virus’ current behavior and long-term health consequences are still poorly understood, imparting urgency to disease control efforts. The CDC travel advisory for the country of interest by our international health elective recommends the following:
Women who are pregnant should not travel to areas in which there is known vector-borne disease;
Women who are pregnant should use condoms or not have sex (vaginal, anal, or oral) during the pregnancy with a male who has been exposed to a Zika-infected area;
Women and men who are trying to become pregnant should consider the risks of a Zika virus infection and strictly follow steps to prevent mosquito bites;
Men who traveled to or live in an area with Zika, and who have a pregnant partner, are recommended to use condoms or not have sex (vaginal, anal, or oral) during the pregnancy.
Reflecting on my clinical encounter with the Puerto Rican male who commutes regularly between known-Zika infected areas and the imminently vector-infected United States, I wonder if he is aware that he poses a risk. Does he believe, as so many often do, that he could not possibly be the one to acquire or sexually transmit an infection? Has he considered the possibility that he could serve as a viral reservoir?
In light of current evidence regarding Zika virus disease and the significant risks, I agree with my mentor’s decision to limit medical student international travel to Zika-infected areas. And I ask myself and readers, what is the responsibility of medical professionals in regards to communicable disease containment?
Thomas DL, Sharp TM, Torres J, et al. Local Transmission of Zika Virus — Puerto Rico, November 23, 2015–January 28, 2016. MMWR Morb Mortal Wkly Rep 2016;65place_Holder_For_Early_Release:154–158. DOI: http://dx.doi.org/10.15585/mmwr.mm6506e2
Oster AM, Brooks JT, Stryker JE, et al. Interim Guidelines for Prevention of Sexual Transmission of Zika Virus — United States, 2016. MMWR Morb Mortal Wkly Rep 2016;65place_Holder_For_Early_Release:120–121. DOI: http://dx.doi.org/10.15585/mmwr.mm6505e1
Simeone RM, Shapiro-Mendoza CK, Meaney-Delman D, et al. Possible Zika Virus Infection Among Pregnant Women — United States and Territories, May 2016. MMWR Morb Mortal Wkly Rep. ePub: 20 May 2016. DOI: http://dx.doi.org/10.15585/mmwr.mm6520e1
Lightening is a beautiful white mustang who enjoys back massages. He loves being around his older brother Lincoln, but shies away from people. Lightening came to Hopewell Ranch in Michigan a few years ago, after barely escaping death. He was abused by his previous family, who disciplined him with a metal two-by-four and cracked his skull. Then they tried to starve him to death. Fortunately for Lightening, he was rescued and became a therapy horse at Hopewell Ranch.
What is equine therapy? Horses like Lightening, with troubled pasts, are used in unique psychotherapy for women and children recovering from domestic violence, cancer patients, veterans, and the list goes on. Equine therapy can also be used for professional development, by teaching the importance of using body language rather than verbalization to elicit responses.
Recently I had the opportunity to visit Hopewell Ranch and participate in one such professional development session. Having never been around horses in my life, I was quite nervous prior to the session. As soon as I stepped in the arena, the horses took notice and the silence between us was powerful, but made me even more nervous. The horses studied my body language, determined that I was not going to harm them, and slowly came over to me. While I was still very cautious, the gentle nature of the horses helped calm my nerves.
After the horses got to know me, I was tasked with identifying some of their personality characteristics based on their reactions to my touch or command. Lincoln, another beautiful Mustang, was clearly the leader of the herd and quite protective of Lightening, who was very nervous and cautious around strangers. Responding to my touch, Lincoln remained steadfast and was no longer nervous around me; however, Lightening continued to shy away from me and recede into the shadow of his brother.
Next, I was placed on a team in order to perform a physical exam on Lincoln, our assigned horse, and finally, we were tasked with getting him to maneuver through a self-made obstacle course. Each task focused on cultivating different skills, such as learning to read body language, working in a team, and leading. Physicians are often required to read a patient within the first 30 seconds of entering the exam room. They must be able to work well in a team and step back when necessary so others can get the job done. A physician must also exude confidence as a leader so a patient has confidence in him or her; equine therapy helps integrate all of these important physician skills.
The most powerful part of this session for me was, again, the silence. Many times, we take speech for granted and believe that because patients can verbalize their thoughts and feelings, they will tell us everything we want to know. However, working with these horses, particularly Lightening, revealed to me the necessity of gaining the trust of my patients. If there isn’t a trusting patient-doctor relationship, they will not feel comfortable sharing their life circumstances or the challenges that need to be overcome to successfully implement therapy. For example, a patient may be homeless, abused, or depressed, but there may not be outward signs at first glance. Learning to read a patient and being able to get him or her comfortable enough to share information are great assets to have in the physician tool belt, because they will help make accurate diagnoses and enable successful treatment.
Beyond professional development, equine therapy is an incredible resource for an array of psychotherapy candidates including, but not limited to, addicts and the handicapped. The founder of Hopewell Ranch, Jodi Stuber, has an incredible story of her own that led her to open this ranch. She lost her daughter at five months in utero, but named her Hope, and then decided to name the ranch after her. In Hope’s memory, Jodi has helped people fight drug addiction, has helped cancer victims learn to ride and experience joy while they endure intensive chemotherapy, and has helped children faced with abuse and disabilities feel empowered, all through the teachings of horsemanship.
Equine therapy is a lesser known, but phenomenal, therapeutic method, and my first experience with Lincoln and Lightening will definitely not be my last. I encourage everyone to seek out equine therapy – for fun, for mental health, and for professional growth and development.
“I succeeded in discovering the cause of generation and life; nay, more, I became myself capable of bestowing animation up on lifeless matter.” – Dr Victor Frankenstein, Frankenstein (2)
Frankenstein is a science fiction novel published by British author Mary Shelley in 1818 that has become an integral part of modern day culture. It follows a Swiss scientist named Dr Victor Frankenstein who becomes obsessed with alchemy and the idea of creating life. His indelible curiosity gradually leads him down the path towards atrocious experiments in the name of science, to the point where he creates a creature – a ‘monster.’
This novel, which has captured our imaginations since its release almost two centuries ago, has led to several famous film adaptations and has become one of the cornerstones of the Horror genre even to the present day.
The inspiration for this novel came from the early 1800s when scientists awed audiences with their ability to use electricity to stimulate the nerves of dead animals, a process called galvanism (1). In 1803 the body of murderer George Foster was attached to a large battery, and witnesses tell us that ‘the adjoining muscles were horribly contorted, and the left eye actually opened’ (3). It was during this era that science started to take over the reins, stepping onto its pedestal as the fountain of knowledge.
Interestingly, the subtitle of Frankenstein is ‘Modern Prometheus’ (3). Prometheus is the Greek God who brought knowledge to humanity, and later paid for his ‘crime’ through eternal torment. In a similar fashion, Victor Frankenstein brings further knowledge to humanity through his obsession with the life sciences, leading to his creation of a ‘monster’ that ultimately torments him to his dying day. The novel, despite being written at a time when science was just learning to walk, is as relevant today as it was when first published. Yes, it may just be a work of fiction, but the deeper warnings contained within its fine pages speak to us in a way that no scientific journal can.
Frankenstein reminds us that the humanities are the seat belt for the sciences. They have been there to remind us of our morals when all we want to indulge in is our supreme power as human beings. They remind us to stay humble, to think and to question, and not merely to set fire to everything that surrounds us.
History is littered with examples of how scientific discoveries can lead us astray. From the splitting of the atom, which led to the creation of nuclear weapons, to the rise of technology, which has led to the dehumanization of everyday life. But of course, this is a simplification. Science has also given us so much that we now take for granted: organ transplants, heating, the latest iPhone, the very roof over our heads. Science has given us our healthy years, filled with food, shelter, safety and comfort. What Frankenstein highlights is our human desire to go further; to extend our years beyond our imagination, so that not only do we never die, we never grow old either. This hubris is perhaps part of human nature.
What Frankenstein teaches us is that we must take responsibility for our creations, and remember that every gleam of hope also betrays a darker path; ultimately, it is not the ‘monster’ that leads to his masters’ demise, but the lack of empathy and responsibility that is displayed. By continually digging deeper and deeper, searching for a way to transform the cells that create us and the organs that give us life, we must not forget the power that lies in our hands, the ever-human desires of greed and selfishness that can take over our quest.
“I might in process of time, renew life where death had apparently devoted the body to corruption” – Dr Victor Frankenstein, Frankenstein (2)
Many may question how relevant such warnings are in the present day. Perhaps these messages do not apply to our times. Very few of us would turn our backs upon science, casting our technologies aside and turning to the fire to heat our food and the rock to give us shelter. The issues that Frankenstein brought up, of using nature to bring about life, can be found within any hospital across the world. The use of the defibrillator – a device that uses electricity to shock the heart back into rhythm – could be described as the answer that Frankenstein worked so hard to find – to bring people back from the dead, to introduce life so to speak. Would one call this abominable?
Perhaps we are being unfair to Frankenstein – looking at ourselves as medical students and doctors, how many of us would not do the same as him; sitting hours within a cramped room, reading textbook after textbook, trying discover the intricacies of the human body: how does it breathe, how does it sleep, how does it eat, how does it live? Isn’t this what we do every day – delve deep into the human body so that we can learn how to shock it back to its original state?
We can choose to see both ourselves and Dr Victor Frankenstein as lights that shine onto pathways of future knowledge, discovering new cures and assembling fresh treatments along the way. But we must remember that we cannot rely on science alone to answer all of our problems. Ultimately, science cannot work in a lab by itself. It must work within the context of our greater society, and it must be made morally accountable for its actions. By continuing one’s endeavors out of pure selfishness and greed, one may tread down a path from which there is no return. In the end, it is the monster created from Frankenstein’s obsessions that kills him, and this can serve as a warning to us all.
“We can only give away to others what we have inside ourselves”-Wayne Dyer
Empathy is the ability to understand and experience life from another person’s perspective, which allows an individual to care for others in a genuine way. In medicine, it is arguably one of the most crucial qualities required to be a good doctor. Research shows that empathetic doctors are perceived as better caregivers, and are less likely to face malpractice suits. (1-4) In another study, which looked at how physicians’ empathy affected clinical outcomes for diabetic patients, it was found that the physicians perceived as more empathetic were more likely to have patients with blood sugars and cholesterol levels under control. (5)
Demonstration of caring and altruism during the medical school application process is almost essential for entry. However, several studies have shown that student empathy is negatively affected by medical education, particularly on entering the clinical years of training. (4, 6, 7) Various factors have been explored to explain this. The higher workload of the clinical years, exam pressures, as well as facing the realities of medicine on the wards (as opposed to previously idealised media images), could all be contributing to the phenomenon.
Moreover, medical students come from a background of overachievement, and stress and anxiety can result from not performing to the standards they expect of themselves. (4) Perhaps as medical students we have also learnt to put on a mask of compassion, kindness and emotional distance to protect ourselves from the realities of life; or maybe it is emotional blunting from just meeting too many ‘people with problems’. (7) Whether the reason for our rise in cynicism is attributed to one or all of these explanations, it seems apparent that the care and compassion we are able to show to patients is primarily associated with our own mental state. With a continuous backdrop of studying and time pressures, the stresses of all life events are heightened.
There has been a large amount of research into the stress, burnout rates and psychological consequences of medical school training. In one multicentre study at American medical schools, burnout was found to be common amongst medical students, and it increased by year of study. (8) The general consensus is that the medical school experience is challenging and demanding, requiring resilience and a balanced lifestyle.
Could medical schools provide more support to ensure students are well equipped to face a career filled with emotionally demanding situations, whilst maintaining the levels of empathy and emotional understanding crucial for strong doctor-patient relationships? All schools offer some level of student support, such as counselling sessions for those students that are experiencing mental difficulties or life challenges. Unfortunately, it has been shown that a clear stigma continues to exist against mental health and guidance in simple life matters. This has been described as “the hidden curriculum”, a culture that exists where doctors and students are led to believe that we are invincible and cannot become ill, either mentally or physically. (9) Often the first signs of vulnerability to mental health issues manifest at medical school, which actually leads to breakdown much later on. (10) Rather than allowing our future doctors to reach their breaking point before seeking help, we could build strong foundations and encourage introspection alongside academic learning. This would help our medical students and doctors truly reach their potential.
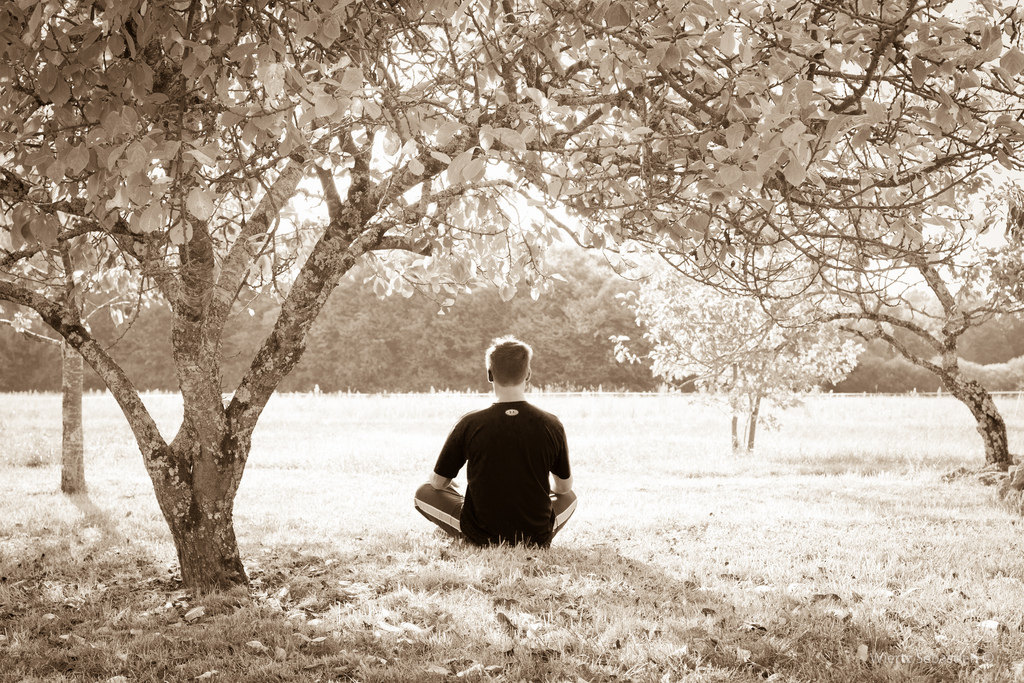
One avenue that has been explored to prevent ‘compassion fatigue’ and burnout is through the practice of mindfulness meditation. One study found that post-intervention levels of anxiety and depression were significantly reduced. (11) Mindfulness is currently taught at 14 medical schools and is continually gaining popularity. The University of Rochester School of Medicine and Dentistry (USA) and Monash Medical School (Australia) are unique in that they have fully integrated mindfulness into their core curricula. (12) One study found statistically significant reductions in tension-anxiety in students on a mediation-based stress reduction (MBSR) program (from 14.5+/-7.2 pre-intervention to 12.4+/-7.0 post-intervention) in comparison to controls (11.3+/-6.3 pre-intervention to 13.4+/-6.9 post-intervention). (13)
Mindfulness is a process to become more conscious of the present moment in order to manage thoughts, feelings and strong emotions. (14) Although it was historically known as a Buddhist practice, with the aim to alleviate suffering and cultivate compassion, it can be practised without spiritual or religious affiliation. In the late 1970s, Jon Kabat-Zinn, a physician at the University of Massachusetts Medical Centre, developed Mindfulness-Based Stress Reduction (MBSR), which takes away the esoteric aspects of the practice while retaining the core elements. This has gained considerable popularity, particularly in the field of pain relief. (15)
A study into the effects of meditation practice on the brain, conducted at Harvard School of Medicine, found that with meditation there was increased gray matter in the frontal cortex, an area associated with working memory and executive decision-making. There was also thickening of three key regions displayed in the table below. (16)
Furthermore, the amygdala, the area of the brain associated with the fight-or-flight response, and thus a key contributor to feelings of anxiety or stress, became smaller. (16) A second study by the same group found that practice for only 8 weeks appears to enhance regions of the brain associated with memory, sense of self, empathy and stress. (17)
Medical school and life as a doctor is a demanding career path. Thus, it can be argued that it is the responsibility of medical educators to both equip students with the academic knowledge required and the emotional intelligence to handle the day-to-day challenges. Mindfulness offers a method to teach medical students how to practically handle stressful emotions and situations, which helps them to become more centred, caring and empathetic. We can only give as much as we have, so it seems intuitive that students who are happier and mentally strong will provide better patient care. The evidence for mindfulness practice is very encouraging and it is interesting to see that two medical schools have already incorporated these practices into their curriculum.
Will mindfulness become as core to the medical school curriculum as the study of anatomy? If we value the mind as much as we do our bodies, then maybe it should.
1. Halpern J. What is clinical empathy? Journal of general internal medicine. 2003;18(8):670-4.
Levinson W, Roter DL, Mullooly JP, Dull VT, Frankel RM. Physician-patient communication: the relationship with malpractice claims among primary care physicians and surgeons. Jama. 1997;277(7):553-9.
Brownell AKW, Côté L. Senior residents’ views on the meaning of professionalism and how they learn about it. Academic Medicine. 2001;76(7):734-7.
Newton BW, Barber L, Clardy J, Cleveland E, O’Sullivan P. Is there hardening of the heart during medical school? Academic Medicine. 2008;83(3):244-9.
Hojat M, Louis DZ, Markham FW, Wender R, Rabinowitz C, Gonnella JS. Physicians’ empathy and clinical outcomes for diabetic patients. Academic Medicine. 2011;86(3):359-64.
Ren GSG, Min JTY, Ping YS, Shing LS, Win MTM, Chuan HS, et al. Complex and novel determinants of empathy change in medical students. Korean journal of medical education. 2016;28(1):67-78.
Hojat M, Vergare MJ, Maxwell K, Brainard G, Herrine SK, Isenberg GA, et al. The devil is in the third year: a longitudinal study of erosion of empathy in medical school. Academic Medicine. 2009;84(9):1182-91.
Dyrbye LN, Thomas MR, Huntington JL, Lawson KL, Novotny PJ, Sloan JA, et al. Personal life events and medical student burnout: a multicenter study. Academic Medicine. 2006;81(4):374-84.
Marshall EJ. Doctors’ health and fitness to practise: treating addicted doctors. Occupational medicine. 2008;58(5):334-40.
Shapiro SL, Schwartz GE, Bonner G. Effects of mindfulness-based stress reduction on medical and premedical students. Journal of behavioral medicine. 1998;21(6):581-99.
Dobkin PL, Hutchinson TA. Teaching mindfulness in medical school: where are we now and where are we going? Medical education. 2013;47(8):768-79.
Rosenzweig S, Reibel DK, Greeson JM, Brainard GC, Hojat M. Mindfulness-based stress reduction lowers psychological distress in medical students. Teach Learn Med. 2003 15(2): 88-92.
Ludwig DS, Kabat-Zinn J. Mindfulness in medicine. Jama. 2008;300(11):1350-2.
Kabat‐Zinn J. Mindfulness‐based interventions in context: past, present, and future. Clinical psychology: Science and practice. 2003;10(2):144-56.
Lazar SW, Kerr CE, Wasserman RH, Gray JR, Greve DN, Treadway MT, et al. Meditation experience is associated with increased cortical thickness. Neuroreport. 2005;16(17):1893.
Hölzel BK, Carmody J, Vangel M, Congleton C, Yerramsetti SM, Gard T, et al. Mindfulness practice leads to increases in regional brain gray matter density. Psychiatry Research: Neuroimaging. 2011;191(1):36-43.
In a world where drug companies and pharmacies remain pervasive, an innovative take on the word “pharmacy” is being developed in Redwood City, CA. A new food pharmacy has just opened up, stocked with fresh fruits and vegetables. Just what the doctor ordered – literally! Instead of paying supermarket prices for these foods, all you need is a prescription from the doctor.
The first of its kind, this food pharmacy is an annex to the existing Redwood City free clinic known as Samaritan House. Patients with type II diabetes can get a prescription for fruits, vegetables, and even fish from a physician, and then pick up the free food at the pantry to help better manage their diabetes. The food is procured and delivered by the Second Harvest Food Bank, which is one of the largest food banks in the nation, feeding almost a quarter of a million people each month. Second Harvest also provides nutritious cooking demos given by local nutritionists1.
This one-year pilot program serves as a reminder that food is often overlooked as a primary method of treatment and prevention; a reminder we might need during our incessant drive to memorize pharmaceuticals and their mechanisms of action. Even when it is known that a patient’s congestive heart failure and diabetes may not be adequately controlled long term by medication alone, oftentimes physicians are strapped when it comes to options. Providing education on proper nutrition to a patient who simply cannot afford fruits and vegetables remains the passive and limited option, whereas food pharmacies such as Samaritan House are active steps in the right direction.
My favorite online resource, Wikipedia, calls gambling, “wagering of money or something of value (referred to as “the stakes”) on an event with an uncertain outcome with the primary intent of winning additional money and/or material goods. Gambling thus requires three elements be present: consideration, chance and prize.”[1] It’s a funny quirk of medical student life that we all involve ourselves in gambling during our final year. The National Residency Matching Program (NRMP) can certainly fit the definition above. The med student wagers their future (“something of value”) on the Match (“an event with an uncertain outcome”) with the goal of finding the program that best suits them (“with the primary intent of winning”). The risk involved is certainly a calculated risk, as the give-and-take of applying, interviewing, and ranking allows us the opportunity to influence the outcome, but it is a risk nonetheless. In fact, it’s worth noting that much of the NRMP data was analyzed by Anna-Maria Barry Jester on the FiveThirtyEight blog last year. The major takeaway of her work was that while the system may very slightly favor the student, at the end of the day, it is the Match’s algorithm that decides.[2]
Fourth year med students are now receiving their “prizes” after going through the “consideration” and “chance” phases of the Match. As a 3rd year med student, I’m firmly rooted in the consideration phase. I’ve already decided my future specialty (family medicine), which is more than some can comfortably say, but now I have 500 programs to sort through, and how can anyone possibly decide where to apply? The consideration phase of my gamble on the Match is just as much of a lottery as anything. Sure, I get to make the final choices, but if there is a perfect program, how do I know it’s not the one I left off my list? It’s a familiar process at least, since it is similar to applying to medical school in the first place. I sent my applications out nationwide, to both osteopathic and allopathic schools. While the system didn’t rely upon an algorithm to decide, the stakes were nearly as high, with just as much uncertainty.
The process of sifting through residencies, though, is better left for another day. Currently, I just stand back and watch as my older brothers and sisters plan their futures. I’m both envious and wary. Certainly it would be nice to know, to have a clear objective. There is a lot of security in certainty. Then again, there is a reason the casinos are always so full in Las Vegas. People love the allure of any game of chance. When the dice are rolled, in that brief moment before the outcome is known, everyone has the potential to be a winner. No one puts a program as number one on their rank list hoping they aren’t selected to go there, just as no one places a bet on number 17 in roulette hoping the ball lands elsewhere.
I’m looking forward to the Match next year. I like to play the odds, always hoping that my number comes up. Luckily, while I may have no say in what cards are dealt in poker, I do have a say in how the Match ends. I get to meet with programs and all the people who populate them. I get to talk about my passions and plans and hope they get a feel for who I am on those interview days. And when I place my rank list, whatever choices I make, I hope I’ve done enough to pick a place that wants me just as much. When the Match algorithm runs, churning out the yes’s and no’s, I hope my number comes up.
Meet Laura Matsen Ko, orthopedic surgeon, avid runner/skier/hiker/cyclist, and new mother to a beautiful baby boy, Logan. Laura and her husband, both orthopedic surgeons at Orthopedic Physician Associates (opaortho.com), practice and adventure in the Pacific Northwest. Together, they developed the website, seattlejointsurgeons.com, which allows patients to access comprehensive and accurate information on orthopedic care.
I met Laura recently on Instagram via a post shared by Oiselle (oiselle.com), a Seattle-based women’s running apparel store named after the French word for bird. In the post, photographed by Kevin, Laura is captured as a pregnant backcountry skier posed on the summit of snowy Mt. Baker. A flurry of follow requests, instant messages, and emails between us quickly snowballed into a cross-country friendship. Our easy rapport is not unexpected considering our shared passions. We are both passionate about helping injured athletes (and specifically pregnant athletes) get back to their sports as soon as possible. After learning of my research interests in antenatal exercise, Laura agreed to a semi-formal interview about her background and experiences related to exercise during pregnancy.
First, tell me a little about yourself. I did some Instagram sleuthing and noted scrubs, ortho, a lot of snow, and Thomas Jefferson.
I was born and raised in Seattle, Washington. I went to Whitman College in Walla Walla, WA where I enjoyed being an outdoor leader on backcountry ski trips and mountaineering trips. My senior year I decided to go out for Cross-Country, and surprised myself by placing 9th at Nationals (D3). Then I bike raced that spring and got 2nd at Nationals (D2). That was a huge surprise and a thrill.
I went to medical school in Portland, Oregon at Oregon Health and Sciences University (OHSU) and continued on at OHSU in an Orthopedic Surgery residency. I did two Ironmans while I was there, including qualifying for, and finishing, the world championship in Kona, HI.
About that time I got to meet my husband who was a year behind me in the Orthopedic Residency, and I finally convinced him to go for a real date with me after one of our rainy runs together. Throughout residency we trained for various marathons together and enjoyed active vacations; anything from cycling to backcountry skiing.
After we finished residency, we headed to Philadelphia. I did a fellowship in Adult Reconstruction. I chose the field of hip and knee joint replacement surgery because it gives me the opportunity to help people return to the activities they enjoy using surgery and personalized rehabilitation.
How many years have you been a backcountry skier and mountaineer?
My father and older brother taught me in my teenage years. We had been backpacking our whole lives, they had been climbing, and I always aspired to go out with them. When I was 13 I took a year-long course with my Dad to learn how to safely rock climb, mountaineer, snow camp, and manage avalanche risk and rescue. That winter my brother took me out in the backcountry and I got stronger and smarter. That summer we climbed five Washington volcanic peaks including Mt Rainier.
What kind of role does skiing have in your life?
Backcountry skiing is a wonderful treat—unlike running it does take a bit of equipment and a bit of driving but it’s totally worth it! I love getting out into the wilderness without anyone around. I equally love the hiking up (“skinning” up) the mountain as much as the fresh, sweet turns on the way down!
Tell me about your pregnancy.
Logan was my first pregnancy. I have always been active, and continuing my activity seemed right to me. I bike-commuted to my work at the hospital, rain or shine, which was about a 15-mile commute. I did this through my second trimester, and then we decided it was too high of a risk to continue cycling due to the short and often rainy dark days in Seattle. My OB, husband, and father all pushed me to stop bike-commuting. I ran up to two weeks prior to him being born. I skied two days before he was born—in bounds alpine one day and three days of very rigorous backcountry skiing. These were about 6 hour days of hiking hard uphill and then skiing down in fresh powder. It was so fun to feel like I was sharing this experience with Logan.
Multi-night mountaineering trip in the Washington Cascades with husband Kevin at 18 weeks gestation.Hike with my Dad at 19.5 weeks gestation.Seattle Half Marathon at 32 weeks gestation. Time: 2:00.
The day I went into labor I did elliptical and weights and performed a major total hip revision surgery. Throughout the second half of my pregnancy I had some issues with SI joint and foot pain, but in general my body held up well.
I did a lot of research about heart rates, but the data seemed inconsistent.
Laura’s difficulty navigating antenatal exercise guidelines is not surprising. A study by Lieferman (2012) demonstrated that almost half of medical providers (48%, N=89) were unfamiliar with current national exercise guidelines for pregnant women and half of respondents advised a reduction in exercise in the third trimester, even for uncomplicated pregnancies. Concurrently, a 2006 study demonstrated that about half of surveyed obstetricians recommended heart rate maximums and a reduction in exercise load during the third trimester—two policies not specified in current guidelines (Entin, 2006).
The American College of Obstetrics and Gynecology (ACOG) and the U.S. Department of Health and Human Services recommend that healthy pregnant and post-partum women engage in 30 minutes of moderate intensity exercise for most, if not all, days of the week (ACOG, 2015; DHHS, 2008). Pregnant women who habitually perform vigorous-intensity aerobic activity may engage in higher intensities under the guidance of a medical provider. Heart rate maximums are no longer indicated. Instead, pregnant women use ratings of perceived exertion to monitor their exercise intensity. For most women, moderate effort is comparable to a brisk walk, at an intensity one can maintain for hours. It should result in heavy breathing, but not so much that the exerciser is unable to hold a short conversation. Vigorous activity, on the other hand, should make the exerciser feel short of breath, but still able to speak a sentence.
Obstetrics (OB) providers are encouraged to educate women about the health benefits of exercise during pregnancy. These benefits include improved gestational diabetes control, lower rates of antenatal and post-partum depression, and relief for back pain. There are several absolute contraindications to exercise during pregnancy, including incompetent cervix or cerclage, multiple gestation at risk of premature labor, persistent second- or third-trimester bleeding, and preeclampsia. For a full list of absolute and relative contraindications, consult the ACOG Committee Opinion Number 650 (ACOG 2015). Certain activities are also identified as safe or unsafe. Unbeknownst by Laura, down-hill snow skiing is listed as an activity to avoid due to an inherently high risk of falling and subsequent abdominal trauma.
Laura continues:
I didn’t really follow [the guidelines] after talking with friends and reading. I didn’t do sustained high intensity intervals, but if I was running stairs and my heart rate got up to 165-170 on the way up but dropped to 120 on the way down, I felt that my baby was getting sufficient perfusion. Each mother has a different pregnancy experience and the biggest factor is to listen to your body. Exercise made me feel happy and alive so I kept doing it. Plus pregnancy can do such a warp on body image. Exercise helped normalize my feelings about the changes in my body.
Why do you think it is most important to listen to your body?
We are all so different. As you’ve seen with your med student classmates, we need different amounts of sleep, caffeine, food, exercise, fresh air… so no single guideline will work. We all must strive to learn our bodies.
My physician friend had a 10-lb baby. She was extremely active, and pre-pregnancy she ran and played soccer. Obviously our pregnancy (and delivery and post-partum) experiences were totally different and not fair to compare. She says she tried to play soccer 7 weeks post-partum and she “felt like her uterus was going to fall out.” Another physician friend had a 9 lb baby with a very large head. She was walking over 5 miles a day until she delivered, but is challenged to get back to walking more than a couple blocks now (2 weeks post-partum) after her more traumatic vaginal delivery. A third physician friend who had always been extremely active in basketball and volleyball was placed on bed rest at 22 weeks for all three of her babies.
I never want to be compared to other women or make other women feel that they just didn’t push hard enough because of my activity levels. I’m one person and this was one pregnancy. The next pregnancy could be totally different! These other women are a lot tougher than me—they had a more challenging pregnancy, delivery, and recovery. And they had to be very patient with their bodies.
Did you have any conversations with your OB provider(s) about your exercise practices during the pregnancy?
Yes… some. They thought I was a little nuts but were supportive. Except for the skiing. My OB was a little shocked to hear that I’d been skiing.
In the first couple weeks post-partum I mostly tried to work on some baseline fitness with walking and stairs. I tried to wait until 6 weeks to really increase my activity but I wasn’t able to wait.
Explain the 6 week mark.
Well I was told by my OB and the nurse practitioners to not exercise hard until 6 weeks. BUT I started running at day 16 and as of 4 weeks was up to about 30-40 miles a week with one day of hill repeats and one day of fartleks. I made it to 8 miles in sub 8 pace with a couple 7:30 until around 4 weeks. I think my first race will be a half marathon at 2.5 months postpartum. I’m not going to be the fastest. Partly because of recent pregnancy but also because of sleep deprivation, returning to work, and not having enough time in the day!
16 days post-partum. 7.2 mile run with baby Logan and husband Kevin at 8:37 minute pace.
Do you have any friends who also skied during their pregnancy?
I knew people who were running and rock climbing in their pregnancy and a lot of friends who just stayed fit with walking. I don’t know anyone else who skied during their pregnancy but I’m sure people out there do it! I’d mainly suggest borrowing your father’s huge rain coat and possibly his ski pants because there is no way you’re fitting in your bibs from pre-pregnancy. And don’t push the speed and steepness; mostly enjoy being out there! You don’t want to fall.
There are definitely other pregnant skiers and a few inspired, future Mamas:
On the mountaineering trips, what, if any, issues did you have with harness fit?
Due to the season I didn’t mountaineer in the second half of pregnancy, so it wasn’t an issue. One of my friends got a lower and upper body harness for her pregnant rock climbing trips.
What kinds of emotions did you encounter during your pregnancy when you were not able to do activities that you enjoy?
I found it super frustrating when others placed restrictions on me. My husband quickly found that he had to present my change in activities as a risk/ benefit. When he told me “no more cycling,” I just wanted to rebel. However he did recently have to fix a clavicle fracture on a woman who was 16 weeks pregnant. She got hit while bike commuting. Thankfully her fetus is okay. That story will make me more conservative with my cycling in my next pregnancy.
At 4.5 weeks post-partum I restarted bike-commuting to work for some half days of clinic. It felt amazing to be back out there and I was so much faster with less weight, higher lung capacity, and likely an increased hematocrit.
Is there anything you want to tell future mothers?
Listen to your body and don’t read too much. Wear support stockings if you work on your feet. Know that you will lose the weight. Fast.
Physicians?
Support your patients.
For future and current obstetrics providers, the Canadian Society for Exercise Physiology developed the PARmed-X for Pregnancy, a physical activity readiness medical questionnaire that guides discussions on exercise during pregnancy in an outpatient setting. The form may be accessed online (http://www.csep.ca/cmfiles/publications/parq/parmed-xpreg.pdf) and is useful for most pregnant women. Athletes, however, have sport-specific safety concerns, training goals, and requirements that may be unfamiliar to the average obstetrics provider. These topics may be explored on an as-needed basis during prenatal visits.
A big thank you to Laura Matsen Ko for sharing your inspiring story! Thank you also to my friend Hannah, who initially tagged me in the Oiselle Instagram post.
References
Leiferman, J., Gutilla, M., Paulson, J., Pivarnik, J. (2012). Antenatal physical activity counseling among healthcare providers. Open Journal of Obstetrics and Gynecology, 2, 346-355
Entin, P. L., Munhall, K. M. (2006). Recommendations regarding exercise during pregnancy made by private/small group practice obstetricians in the USA. J Sports Sci Med, 5, 449-458.
American College of Obstetricians and Gynecologists. Physical activity and exercise during pregnancy and the postpartum period. Committee Opinion No. 650. Obstet Gynecol 2015;126:e135–42
U.S. Department of Health and Human Services. 2008 Physical Activity Guidelines for Americans. Department of Health and Human Services Washington, DC; 2008.
Featured image:
Laura Matsen Ko skiing. Photographed by Kevin Ko.
“God, but life is loneliness, despite all the opiates, despite the shrill tinsel gaiety of “parties” with no purpose, despite the false grinning faces we all wear .. Yes, there is joy, fulfillment and companionship – but the loneliness of the soul in its appalling self-consciousness is horrible and overpowering.” – Sylvia Plath (1)
Who amongst us has not felt the hand of loneliness? The first breakup as a teen, the rejection letter lying on the kitchen table, children moving away for the first time, the little cracks in a marriage beginning to show. If loneliness is so widespread, so ‘normal,’ why do we need to talk about it? Aren’t we generally attracted to the more rare and wonderful aspects of life? Aspects like the documentation of odd and wonderful medical conditions, the extremes of human behaviour that we can analyse with such voyeuristic enthusiasm. The topic of loneliness has instead been taken over by the arts; a subject for novelists and philosophers to dissect rather than scientists and clinicians.
Loneliness can be defined in a couple of different ways: emotional and social loneliness. Emotional loneliness occurs in the absence of an attachment figure, while social loneliness occurs in the absence of a social network. Emotional loneliness has been compared to a child’s feeling of distress when they feel abandoned by their parent, while social loneliness is the feeling of exclusion by a child whose friends have left. Thus, loneliness can be described either as a devoid outer world, or an empty inner world.
On the other hand, the cognitive approach suggests that loneliness stems from one’s social expectations not being met. Could it be that through our reliance on social media, our expectations for relationships have become exaggerated? As we scroll through our Facebook feeds, we become an outside observer to the fruitful lives around us; to parties we have missed, weddings we have declined. And so we draw a comparison to our own lives, thinking of ourselves as hollow shells in comparison to these roaring waves we see around us.
But what is the opposite of loneliness? Is it social connection? Is it the number of contacts we display on our phones? The number of parties we are invited to every month? Or the feeling we have of being valued? Is it being able to share a chuckle while watching a movie, reading a novel with a soft hand by your side, or simply being present in another’s life and being acknowledged?
Loneliness is different from solitude. Solitude can be an enlightening experience, leading to increased creativity and growth. Some of the best ideas have come through hours of sitting at an office desk, staring at a piece of paper. Just because more people in today’s society are living alone, does not mean that loneliness is on the rise. We must be careful not to mix these terms together. Loneliness is very different from solitude. Loneliness is the feeling of despair and alienation. It develops from the need for intimacy, and from the feeling of rejection when one fails to find it. It is described as a social pain; what is the equivalent of morphine for the pain of loneliness?
The power of loneliness can be illustrated through the effects of solitary confinement. It has been suggested that prisoners who have been through solitary confinement develop psychiatric disorders such as depression and anxiety, often turning to self-harm as a means of escape. Solitary confinement is described as a form of psychological torture, with one Florida teenager describing his experience as “the only thing left to do is go crazy.” Humans are social creatures. Without stimuli and control, is it any wonder that depression, hypersensitivity, and psychosis develop? This isn’t just an abstract concept that we are talking about, something for the philosophers to discuss at their round tables. It has implications with regards to disease, happiness, and relationships. It can be found in every aspect of our lives, in every infant and every adult – it is something that needs to be examined more closely through our microscopes.
“The most terrible poverty is loneliness, and the feeling of being unloved.” ―Mother Teresa (2)
The topic of loneliness has fascinated novelists, poets, theologians, and philosophers, all attempting to give meaning to this beast. Yet psychoanalyst Shmuel Erlich suggested that the meaning of loneliness remains “an enigma” (3).
The concept of loneliness looks deep at the need for human connection. Through the rise of science and technology, a result on our emphasis on empirical modes of thought, we have gained considerable scientific knowledge and a whirlwind of medical technology. Yet what has happened to the conversation involving spirituality, social customs, and personal relationships? What has happened to the human perspective? Dig as deep as you like into the functions of the human body, the junctions between the cells and the DNA mutations – just remember that the knowledge that is discovered needs to be applied to a living, breathing human being. Can we quantify the despair of loneliness, the cracks of a thirty-year marriage, the grief of a mother who has lost her child? We may spend our lives pursuing wealth and status, but ultimately it is meaning that we all search for in the end.
“Existential aloneness is necessarily a part of serious illness.” – S. Kay Toombs (4)
How does it affect us as doctors?
As healthcare professionals, we are trained to be objective, to look at the statistics, and arm ourselves with the jargon of relative-risk and correlations. But walk into any hospital, and you will not see wards filled with numbers and graphs. You will see vulnerability, the eyes of loss, of angst and fear. You will see people tested to their limits, people whose lives are cracked and crumbling – people who have entered the threshold of loneliness.
Is loneliness a pathological condition? Intolerance for being alone was once a criterion for the diagnosis of Borderline Personality Disorder in DSM-III, while more recently, loneliness was found to increase risk of mortality by up to 26% (5). It can be argued that loneliness can have a purpose in our lives; it can form the path towards self-acceptance, growth and spiritual transcendence. The existential perspective goes so far as to say that loneliness is what it means to be human. It argues that through loneliness, one can begin to question one’s own existence, and thereby create meaning for oneself in a world that has lost all meaning. Western literature paints loneliness as a vital part of being human. It is seen as an obstacle one must climb through during the various experiences of life – through change, bereavement, love and loss. It has been argued that just as joy is made brighter through the experiences of sorrow, loneliness shines a light on the meaning of our life. Yet loneliness has also been linked to alcoholism, depression and suicidal ideation. At what point do we as healthcare professionals need to step in and help someone climb out from this abyss? Where do we draw the line between self-discovery and pathology?
Loneliness can also manifest itself through illness, both physical and mental. The feeling of a broken body, of being a burden on one’s family, can lead to helplessness. Roles that were once worn with pride are now cast aside: the mother, the carer, the provider. These can lead to a loss of self-identity and raise questions about how one can contribute to society. Ultimately, being ill can be an isolating experience, raising questions about one’s reasons for existence and the value of one’s life. As healthcare professionals, it is our duty to guide our patients through this journey. It is our responsibility to help them discover their own meaning for this loneliness, to help them affirm their identity. It is not always distraction or drugs that a patient needs, but an open conversation, which can help patients to gain new perceptions on what it means to be human. The role of the professional is not to provide answers or interpretations, but to listen, to share and to understand. It is a difficult task, filled with uncertainty and anxiety for both practitioner and patient, but it is also human.
We often cast aside people who are deemed lonely; they are the shy recluses, the self-pitying. We suggest that the cure for loneliness is simple: join clubs, create hobbies, meet new people.
By following such advice, we forget something vital: you do not have to be alone to be lonely. It is more than just being independent or respectful of others’ privacy; it is a feeling of distress. Loneliness illustrates our need for human intimacy. So where can we find this painkiller to drug us against such distress? Which specialist will take away our aches and pains? You do not need to be a trained medical professional to combat loneliness. Just remember, Hello is the most powerful word against loneliness.
To the one who set a second place at the table anyway.
To the one at the back of the empty bus.
To the ones who name each piece of stained glass projected on a white wall.
To anyone convinced that a monologue is a conversation with the past.
To the one who loses with the deck he marked.
To those who are destined to inherit the meek.
To us.
– Flood: Years of Solitude by Dionisio D. Martinez (6)
References
Plath, S. 2002. The Unabridged Journals of Sylvia Plath. Anchor Books.
Dionisio, D., Martinez. 1992. Flood: Years of Hope; Years of Solitude; Years of Reconciliation; Years of Fortune; Years of Judgment; Years of Vision; Years of Discourse. 22: 159-162
The in-class assignment was simple: write a short paragraph of your thoughts about narrative medicine. But after ten minutes, my paper was a mess; pen lines angrily crossed out sentences that had been started but not finished, my usually neat penmanship was messy, my vocab unsure. My writing screamed hesitation. After begrudgingly turning in my assignment, I realized just how long it had been since I had written in my journal, which I had left tucked away in a nightstand in my childhood bedroom. I thought it was an appropriate place to leave the book—covered in cheesy flowers with a creased binding—that had chronicled my high school and college years. As I was packing for medical school, it seemed almost off-putting at the time to continue to chronicle the next chapter of my life—what I naively perceived to be the real challenges of medical school—on the same page as my previous entry, in which I complained about the trials and tribulations of learning how to drive stick shift and tackling organic chemistry. Instead, tucked away in my new bedroom, is a leather-bound journal, a gift I received for medical school, emblazoned with the words “FOLLOW YOUR DREAMS.” Every inch of it is covered in cartoon birds. It has been sitting in a drawer since I moved in, untouched.
As I juggle this new chapter as a busy first year med student, that seemingly simple assignment reminds me how much I miss, and clearly need, a nightly journaling routine as my outlet to find peace with my hurried thoughts at the end of a hectic day. It is all too easy to fall into the daily hustle and bustle of med school life such that every day seems almost like the one before. Study, extracurriculars, preceptorship, sleep. Lather, rinse, repeat. All too often, before I fall asleep, I find myself falling into the trap of using my phone to mindlessly relax; catching up on my Facebook newsfeed, scrolling through photos on Instagram—or, if we’re being totally honest here—catching up on celebrity gossip (let’s just say, I’ve definitely been keeping up with the Kardashians). But by the time I “unplug,” my brain is often wired. So much for unwinding.
Yet, even as I write this entry (yes, write, not type!), I understand how relaxing it is to unwind and take the time to process the day’s events with the written word. To really chronicle how every day is not like the one before, but how each day actually brings a new perspective as a result of what I had done that day: conversing with a new classmate, grasping the latest material in class, practicing the hands-on skills I’ve obtained in my preceptorship, etc. I see how important writing about these experiences is for me; to have something tangible to look back upon, years after medical school. To read through each chapter—to remember how I had stumbled when learning to measure blood pressure and take a patient history—just as I reflect now when I read back on my teenage struggles.
It’s important that we, as future physicians, find whatever it is that provides us with this sense of mindfulness, whether it be exercise, meditation, spirituality, etc., and holdon to it. It is through this self-awareness that we can see not only how we have changed, but even more importantly, to find a moment’s peace in the midst of the commotion that each day brings as we pursue careers in medicine.
So, when I go back to my childhood home to visit my family, I’ll be sure to pack up my journal.